Artificial Disc Replacement in Pasadena, CA
A motion-preserving alternative to spinal fusion for the right cervical and lumbar disc patients..
;

Artificial Disc Replacement
If you live in Pasadena and a spine surgeon at Huntington Hospital or somewhere else in town has told you that you need a fusion for your neck or low back, it is worth a second opinion before you let anyone permanently lock two of your vertebrae together. Artificial disc replacement (ADR) is a motion-preserving alternative that did not exist a generation ago, and for the right patient it changes the math entirely. Dr. Kambiz Hannani's West Covina office is roughly 16 miles southeast of Old Pasadena — about a 25 to 30 minute drive down the 210 East to the 605 South to the 10 East — and he has spent more than two decades performing both cervical and lumbar disc replacement for patients across the San Gabriel Valley.
Many of the Pasadena patients we see come in already carrying a stack of MRI films and a fusion recommendation from elsewhere. Some of them turn out to be excellent ADR candidates and leave with a very different plan. Others turn out to need the fusion after all — and they leave knowing why, with the full reasoning explained. The point of the visit is an honest assessment, not a sales pitch.
What is Artificial Disc Replacement?
Between every two vertebrae in your spine sits a disc — a soft, shock-absorbing cushion that lets your spine bend, twist, and absorb load. When a disc wears out, dries out, or herniates, the result is often pain, nerve compression, weakness, and stiffness. The traditional surgical answer has been spinal fusion: remove the bad disc and bolt the two vertebrae together so they move as one. Fusion works, but it eliminates motion at that level, which can place extra stress on the levels above and below over the following years.
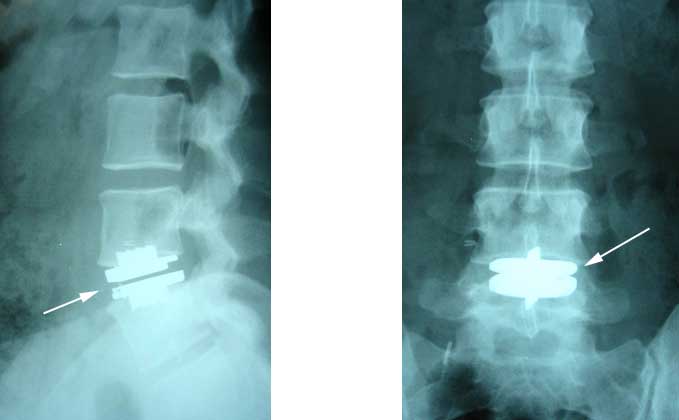
Artificial disc replacement is the alternative. The damaged disc is removed and replaced with an FDA-approved mechanical implant — typically a metal-and-polyethylene device — that preserves the natural motion of the spine. The patient keeps the ability to bend and rotate at that level, and the surrounding discs are spared the extra wear-and-tear they would absorb after a fusion.
ADR vs. Spinal Fusion: The Real Difference
For the right patient, ADR offers meaningful advantages over fusion:
Motion is preserved. The treated level still bends and rotates, which feels more natural and reduces the risk of adjacent segment disease — the long-term breakdown of the discs above and below a fusion.
Faster return to normal activity. There is no waiting for bones to fuse together. Many patients are walking the same day and back to desk work within 2 to 4 weeks.
No bone graft harvest. Fusion often requires harvesting bone from the hip; ADR does not.
Lower long-term re-operation risk at adjacent levels. Multiple long-term studies (5 and 10 years) now show ADR patients are less likely to need a second surgery at a neighboring disc compared with fusion patients.
Fusion still has its place — particularly for patients with significant instability, prior failed surgery, or severe arthritis at the facet joints. The right operation is the one that fits your spine, and that determination requires a careful in-person evaluation with imaging.
Cervical (Neck) vs. Lumbar (Low Back) Disc Replacement
Cervical disc replacement is the more common of the two procedures. It is most often used for patients with arm pain, numbness, or weakness from a herniated or degenerated cervical disc that has not improved with non-surgical care. The procedure is done through a small incision in the front of the neck (anterior approach), the diseased disc is removed, and the artificial disc is implanted in its place. Most patients go home the same day or after one night in the hospital.
Lumbar disc replacement is reserved for a narrower group — typically younger patients with isolated single-level degenerative disc disease in the low back, no significant facet arthritis, and no prior fusion. The lumbar implant is placed through an anterior approach (through the abdomen), which avoids cutting through back muscles and tends to result in less post-operative back pain than a posterior fusion.
Why Patients in Pasadena Choose Dr. Hannani for Disc Replacement
Pasadena is well-served on the medical front — Huntington Hospital is one of the strongest community hospitals in Southern California, USC Verdugo Hills is nearby in Glendale, and City of Hope is a short drive east in Duarte. But artificial disc replacement is a sub-specialized procedure, and not every excellent general spine surgeon performs it routinely. Patients from Pasadena, San Marino, South Pasadena, Altadena, Sierra Madre, and the Bungalow Heaven area come to Dr. Hannani specifically because he has been performing both cervical and lumbar ADR for two decades and can compare the disc-replacement option against fusion in detail — using your actual MRI rather than a generic explanation.
There is also a strong second-opinion culture in Pasadena. Many of our Pasadena patients are professionals — Caltech researchers, Pasadena City College faculty, attorneys, physicians' family members — who have already done their reading and want the surgeon to actually answer their questions. Dr. Hannani's consultations are unhurried for exactly this reason. If you are weighing fusion against ADR, that comparison deserves more than ten minutes.
Getting to Our Office from Pasadena
From most of Pasadena, the simplest route is the 210 East to the 605 South to the 10 East, exiting at Citrus Avenue or Barranca Avenue in West Covina. From Old Pasadena and Caltech the drive is typically 25 to 30 minutes outside of rush hour; from San Marino or South Pasadena, slightly less. The office has free on-site patient parking — no garage hunting, no validation paperwork. If you are coming from the Hastings Ranch side of Pasadena, the 210 East to the 57 South to the 10 West is sometimes faster depending on time of day.
A Patient Story
A 47-year-old architect from South Pasadena came to us last year with a year of left arm pain, numbness in two fingers, and a C5-C6 disc herniation on MRI. She had been told at another practice that she needed a two-level cervical fusion. On review, the C6-C7 level above looked degenerated on imaging but was not the source of her symptoms — and the patient still had excellent disc height and no facet arthritis at C5-C6. She underwent a single-level cervical disc replacement, went home the next morning, was off narcotics in five days, and was back at her drafting table within three weeks. Three years later her motion is preserved and the second level has not progressed.
Who is a Candidate for Artificial Disc Replacement?
Not every patient with disc pain is a candidate for ADR. The best candidates generally:
Have pain originating from a single damaged disc (or two adjacent discs)
Have failed at least 6 weeks of non-surgical treatment (physical therapy, medications, injections)
Do not have severe arthritis at the small joints behind the disc (facet joints)
Do not have significant osteoporosis
Have not had a prior fusion at the same level
Are typically between 18 and 60 years old, though older healthy patients can sometimes qualify
A thorough work-up — including current MRI, dynamic X-rays, and a physical examination — is the only way to know for sure. Patients who are not ADR candidates are not stuck: there are excellent fusion, decompression, and minimally invasive endoscopic options available.
What Recovery Looks Like
Cervical ADR patients are usually walking the same day, eating dinner that night, and home within 24 hours. Most are off narcotic pain medication within a week, driving within 2 weeks, and back to a desk job within 2 to 4 weeks. Heavy labor and contact sports are restricted for about 3 months.
Lumbar ADR recovery is slightly longer because of the abdominal approach. Patients typically stay 1 to 2 nights in the hospital, walk the next morning, and return to light activity in 4 to 6 weeks.
Frequently Asked Questions from Pasadena Patients
How long is the drive from Pasadena to your West Covina office? Typically 25 to 30 minutes outside of rush hour, via the 210 East to the 605 South to the 10 East. From Old Pasadena, San Marino, and South Pasadena it is closer to 25; from Altadena or Sierra Madre, closer to 30. Free on-site parking is available.
Do you take the same insurance plans accepted by Huntington Hospital and other Pasadena providers? We accept most major California insurance plans, including Medicare, Blue Shield, Aetna, Cigna, United, and most PPO products commonly used in the Pasadena area. Cervical disc replacement is now a covered benefit on most of these plans when medical necessity is documented. Our office handles pre-authorization on your behalf — call us with your card and we will verify before your visit.
Can I have my disc replacement surgery done at Huntington Hospital in Pasadena? Dr. Hannani's primary surgical privileges are at Emanate Health in West Covina, where he has operated for many years and where the team is familiar with his ADR technique. He does not currently operate at Huntington. Many Pasadena patients find the slightly longer drive on surgery day a reasonable trade for an experienced ADR surgeon and a familiar OR team — and the West Covina facility is a quiet, low-volume environment compared with a large urban hospital.
I was told I need a two-level fusion. Is that ever appropriate for ADR instead? Sometimes. Two-level cervical disc replacement is FDA-approved and is the right operation for selected patients. Two-level lumbar ADR is more limited. The only way to know is a careful imaging review — bring your MRI on disc to the consultation.
How do I schedule a consultation? Call our office at 626-939-5900 or visit our contact page. Bring any prior MRI or X-ray imaging on disc if you have it — this lets Dr. Hannani give you a meaningful opinion at the first visit.